A 48-year-old male with a 20-year history of heavy alcohol use presents with jaundice, tender hepatomegaly, and confusion. Blood tests show:
AST: 210 IU/L (normal 10–40)
ALT: 90 IU/L (normal 10–45)
What is the most likely mechanism for the elevated AST:ALT ratio in this patient? Explanation: Alcohol metabolism generates acetaldehyde, which damages mitochondria. AST is more concentrated in mitochondria than ALT, so AST levels are disproportionately elevated in ARLD, typically giving an AST:ALT ratio >2.
A 42-year-old female with obesity and type 2 diabetes is found to have hepatomegaly and elevated transaminases. ALT is greater than AST. Ultrasound shows a hyperechoic liver consistent with steatosis. Explanation: In NAFLD, insulin resistance leads to increased lipolysis and elevated circulating free fatty acids. The liver converts these into triglycerides, resulting in fat accumulation (steatosis).
In both ARLD and NAFLD, progression from steatosis to fibrosis involves which of the following key cellular changes? Explanation: Ongoing injury (from ROS, inflammation, lipotoxicity, etc.) activates hepatic stellate cells, which deposit extracellular matrix proteins, causing fibrosis and architectural distortion.
A 45-year-old man with known cirrhosis presents with increasing abdominal distension and new-onset confusion. Blood tests reveal:
Total bilirubin: 48 µmol/L (normal 0–20)
INR: 1.9 (normal 0.9–1.3)
What pathophysiological process best explains his encephalopathy? Explanation: In liver failure, ammonia accumulates due to impaired urea cycle function in hepatocytes. This neurotoxin crosses the blood–brain barrier, leading to cerebral dysfunction and hepatic encephalopathy.
Although ARLD and NAFLD both lead to hepatic steatosis and inflammation, what is the primary upstream driver of liver injury in NAFLD? Explanation: In NAFLD, insulin resistance results in uncontrolled peripheral lipolysis, flooding the liver with free fatty acids. These are converted to triglycerides and generate ROS, driving steatosis and progression to NASH.
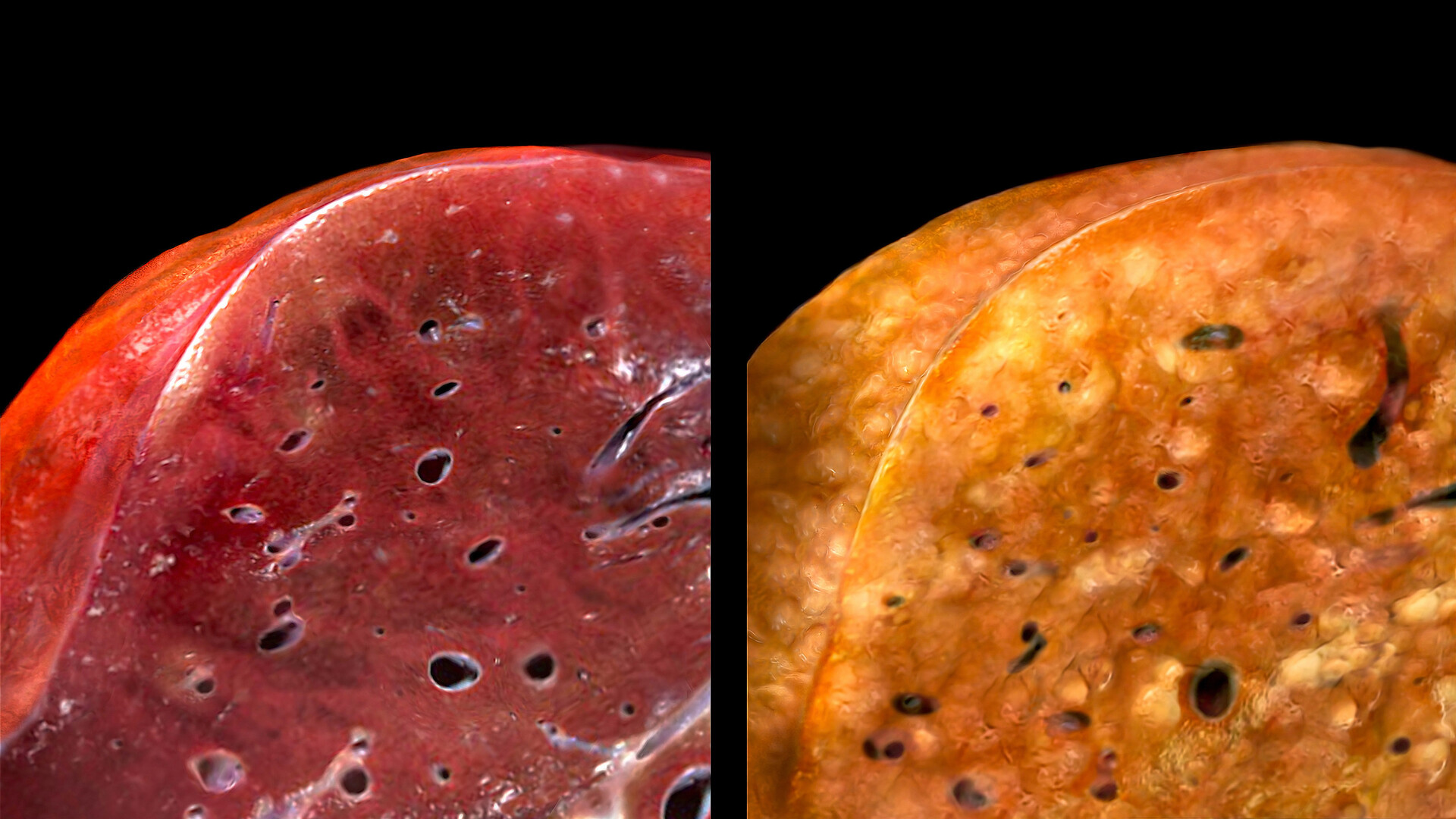 A 5-question quiz exploring the pathophysiology of alcohol-related and non-alcoholic fatty liver disease (ARLD vs NAFLD). Read each clinical scenario and choose the best explanation.
A 5-question quiz exploring the pathophysiology of alcohol-related and non-alcoholic fatty liver disease (ARLD vs NAFLD). Read each clinical scenario and choose the best explanation.
No comments:
Post a Comment